
Page 39 - MDJ Volume 47 Number 2 ( Jul-Dec 2024)
P. 39
Mustafa, et al.: Management of the Impacted Tooth with Dilacerated Roots – A Surgical Challenge
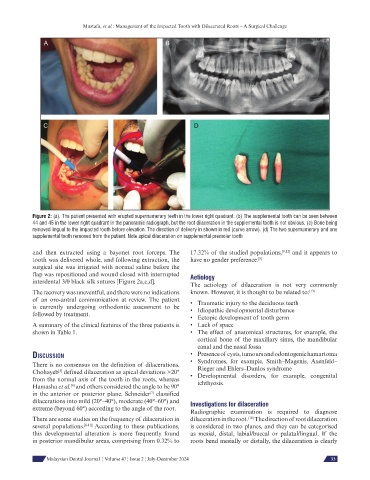
Figure 2: (a). The patient presented with erupted supernumerary teeth in the lower right quadrant. (b) The supplemental tooth can be seen between
44 and 45 in the lower right quadrant in the panoramic radiograph, but the root dilaceration in the supplemental tooth is not obvious. (c) Bone being
removed lingual to the impacted tooth before elevation. The direction of delivery in shown in red (curve arrow). (d) The two supernumerary and one
supplemental tooth removed from the patient. Note apical dilaceration on supplemental premolar tooth
and then extracted using a bayonet root forceps. The 17.32% of the studied populations, [9,12] and it appears to
tooth was delivered whole, and following extraction, the have no gender preference. [5]
surgical site was irrigated with normal saline before the
flap was repositioned and wound closed with interrupted Aetiology
interdental 3/0 black silk sutures [Figure 2a,c,d].
The aetiology of dilaceration is not very commonly
The recovery was uneventful, and there were no indications known. However, it is thought to be related to: [13]
of an oro-antral communication at review. The patient • Traumatic injury to the deciduous teeth
is currently undergoing orthodontic assessment to be • Idiopathic developmental disturbance
followed by treatment.
• Ectopic development of tooth germ
A summary of the clinical features of the three patients is • Lack of space
shown in Table 1. • The effect of anatomical structures, for example, the
cortical bone of the maxillary sinus, the mandibular
canal and the nasal fossa
dIscussIon • Presence of cysts, tumours and odontogenic hamartoma
There is no consensus on the definition of dilacerations. • Syndromes, for example, Smith–Magenis, Axenfeld–
Rieger and Ehlers–Danlos syndrome
[5]
Chohayeb defined dilaceration as apical deviations >20° • Developmental disorders, for example, congenital
from the normal axis of the tooth in the roots, whereas ichthyosis.
[6]
Hamasha et al. and others considered the angle to be 90°
[7]
in the anterior or posterior plane. Schneider classified
dilacerations into mild (20°–40°), moderate (40°–60°) and Investigations for dilaceration
extreme (beyond 60°) according to the angle of the root.
Radiographic examination is required to diagnose
There are some studies on the frequency of dilaceration in dilaceration in the root. The direction of root dilaceration
[10]
several populations. [8-11] According to these publications, is considered in two planes, and they can be categorised
this developmental alteration is more frequently found as mesial, distal, labial/buccal or palatal/lingual. If the
in posterior mandibular areas, comprising from 0.32% to roots bend mesially or distally, the dilaceration is clearly
Malaysian Dental Journal ¦ Volume 47 ¦ Issue 2 ¦ July-December 2024 33