
Page 15 - MDJ 2022 Jan-Jun, Volume 45 Number 1
P. 15
Orthodontic Mini Implant: Malaysian perspective
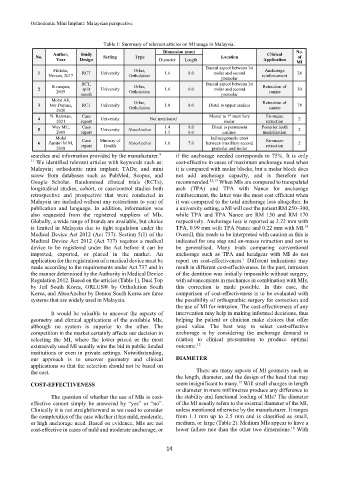
Table 1: Summary of relevant articles on MI usage in Malaysia.
Dimension (mm) No.
Author, Study Clinical
No. Setting Type Location of
Year Design Diameter Length Application
MI
Buccal aspect between 1st
Fitrisha, Orlus, Anchorage
1 RCT University 1.6 8.0 molar and second 24
Noreen, 2017 Ortholution reinforcement
premolar
RCT, Buccal aspect between 1st
Sivarajan, Orlus, Retraction of
2 split University 1.6 6.0 molar and second 30
2019 Ortholution canine
mouth premolar
Mohd Ali, Orlus, Retraction of
3 Nor Dayana, RCT University 1.8 8.0 Distal to upper canines 78
2020 Ortholution canine
st
N. Rahman, Case Mesial to 1 maxillary En-masse
4 University Not mentioned 2
2021 report molar retraction
Wey MC, Case 1.4 8.0 Distal to permanent Posterior teeth
5 University AbsoAnchor 2
2008 report 1.5 6.0 canines. mesialisation
Mohd Infrazygomatic crest
Case
6 Zambri M M, report Ministry of AbsoAnchor 1.6 7.0 between maxillary second En-masse 2
retraction
Health
2018 premolar and molar
searches and information provided by the manufacturer. 9– if the anchorage needed corresponds to 75%. It is only
11 We identified relevant articles with keywords such as: cost-effective in cases of maximum anchorage need when
Malaysia; orthodontic mini implant; TADs; and mini it is compared with molar blocks, but a molar block does
screw from databases such as PubMed, Scopus, and not add anchorage capacity, and is therefore not
Google Scholar. Randomised clinical trials (RCTs), recommended. 12,13 When MIs are compared to transpalatal
longitudinal studies, cohort, or case/control studies both arch (TPA) and TPA with Nance for anchorage
retrospective and prospective that were conducted in reinforcement, the latter was the most cost efficient when
Malaysia are included without any restrictions to year of it was compared to the total anchorage loss altogether. In
publication and language. In addition, information was a university setting, a MI will cost the patient RM 250–300,
also requested from the registered suppliers of MIs. while TPA and TPA Nance are RM 150 and RM 170
Globally, a wide range of brands are available, but choice respectively. Anchorage loss is reported as 2.22 mm with
is limited in Malaysia due to tight regulation under the TPA, 0.99 mm with TPA Nance and 0.22 mm with MI.
14
Medical Device Act 2012 (Act 737). Section 5(1) of the Overall, this needs to be interpreted with caution as this is
Medical Device Act 2012 (Act 737) requires a medical indicated for one step and en-masse retraction and not to
device to be registered under the Act before it can be be generalised. Many trials comparing conventional
imported, exported, or placed in the market. An anchorage such as TPA and headgear with MI do not
application for the registration of a medical device must be report on cost-effectiveness. Different indications may
1
made according to the requirements under Act 737 and in result in different cost-effectiveness. In the past, intrusion
the manner determined by the Authority in Medical Device of the dentition was initially impossible without surgery,
Regulation 2012. Based on the articles (Table 1), Dual Top with advancements in mechanics in combination with MIs,
by Jeil South Korea, ORLUS® by Ortholution South this correction is made possible. In this case, the
Korea, and AbsoAnchor by Dentos South Korea are three comparison of cost-effectiveness is to be evaluated with
systems that are widely used in Malaysia. the possibility of orthognathic surgery for correction and
the use of MI for intrusion. The cost-effectiveness of any
It would be valuable to uncover the aspects of intervention may help in making informed decisions, thus
geometry and clinical applications of the available MIs, helping the patient or clinician make choices that offer
although no system is superior to the other. The good value. The best way to select cost-effective
competition in the market certainly affects our decision in anchorage is by considering the anchorage demand in
selecting the MI, where the lower priced or the most relation to clinical presentation to produce optimal
12
extensively used MI usually wins the bid in public funded outcome.
institutions or even in private settings. Notwithstanding,
our approach is to uncover geometry and clinical DIAMETER
applications so that the selection should not be based on
the cost. There are many aspects of MI geometry such as
the length, diameter, and the design of the head that may
15
COST-EFFECTIVENESS seem insignificant to many. Will small changes in length
or diameter in mere millimetres produce any difference to
The question of whether the use of MIs is cost- the stability and functional loading of MIs? The diameter
effective cannot simply be answered by “yes” or “no”. of the MI usually refers to the external diameter of the MI,
Clinically it is not straightforward as we need to consider unless mentioned otherwise by the manufacturer. It ranges
the complexities of the case whether it has mild, moderate, from 1.1 mm up to 2.5 mm and is classified as small,
or high anchorage need. Based on evidence, MIs are not medium, or large (Table 2). Medium MIs appear to have a
16
cost-effective in cases of mild and moderate anchorage, or lower failure rate than the other two dimensions. With
14